An elderly male presents with constipation. A KUB is ordered and this is what is seen (understandably it’s a poor quality film, but it’s the actual film that was obtained):

The glaring abnormality is the coffee-bean-shaped colon; this patient has a sigmoid volvulus.
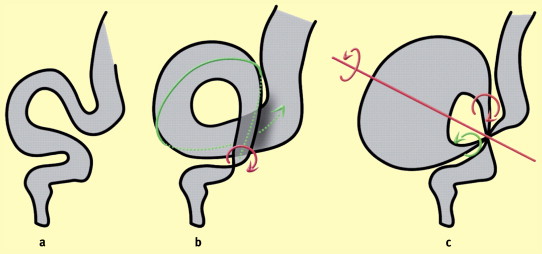
Sigmoid volvulus is a cause of large bowel obstruction and occurs when the sigmoid colon twists on the sigmoid mesocolon.
It has been described as far back as the days of Hippocrates, when he wrote about treatment for volvulus being an injection of a large quantity of air into the intestines via the anus. He further recommended insertion of a suppository that was ’10 digits’ long (modern proctoscopic decompression uses instruments nearly the same exact length!).
It is more common in the elderly (as opposed to a cecal volvulus, which is classically found in younger patients).
The underlying cause may be dietary (diets that are high in fiber can predispose by causing colonic elongation), chronic constipation, medication-related, etc.
Symptoms are the same as that of a large bowel obstruction: abdominal bloating, constipation, nausea/vomiting, etc.
Patients are at high-risk for perforation and/or ischemia.
Previously, laparotomy was the only therapeutic option. Nowadays, detorsion using a rigid proctoscope or flexible sigmoidoscope may be done. This is a great option in patients who cannot tolerate laparotomy or as a temporizing measure. Without surgical correction, recurrence rates may be as high as 90% (and mortality rates as high as 40%).
If detorsion is successful and no ischemia or gangrenous bowel is encountered, a rectal tube can be left and elective resection scheduled. Patients with signs of sepsis (fever, leukocytosis, peritonitis) should be taken directly to the OR for exploration.
Here’s our patient’s x-ray the next day. The rectal tube has decompressed the volvulus!




{kind=link}