
I work in a combination of private practice and academics. Each carries its own advantages and drawbacks, but it’s hard to argue with the joy that comes from teaching a new procedural skill to a welcoming student. As long as the person is open to learning, it will benefit them in their career, and it can be done safely, taking time to help someone learn brings me immense pleasure. To that end, a relatively stable patient presented with an acute overdose. After failing to respond to naloxone and being unsure what he might have ingested, the decision was made to intubate for airway protection.
I was working with a student who has a penchant for learning. She’s one of those rare birds who welcomes any nugget of information you can share with her. So of course as soon as I recognized that this patient needed an airway, I called her and offered to help walk her through it. She bounced up to the resuscitation room and happily prepped for the intubation. I was by her side the whole time but once she passed the cords and I confirmed placement (auscultation, rising sats, etc) I left the patient in the hands of the respiratory therapist to secure the ET tube.
A few minutes later, I pulled up the x-ray and here is what I saw:
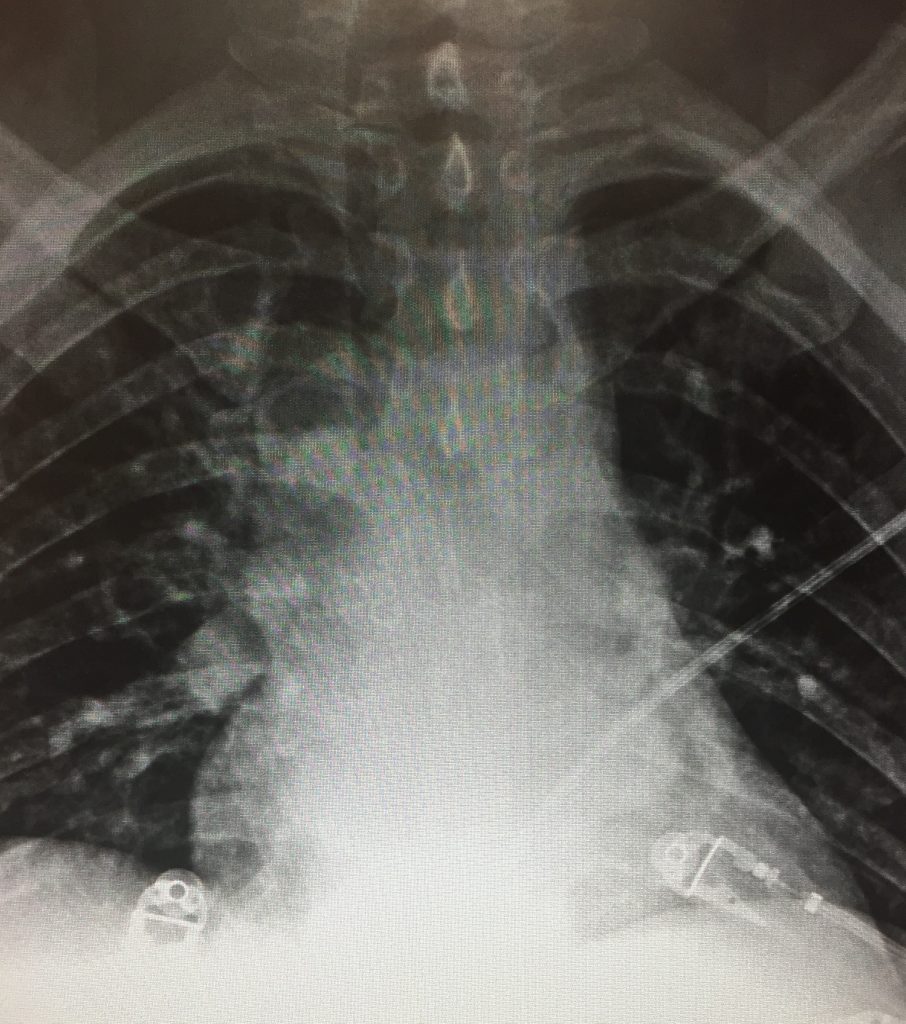
Hmm. Maybe this was a pre-intubation x-ray. I checked the time. It wasn’t. I poked my head in the door and sure enough there was a tube secured there. So where the dickens was it?

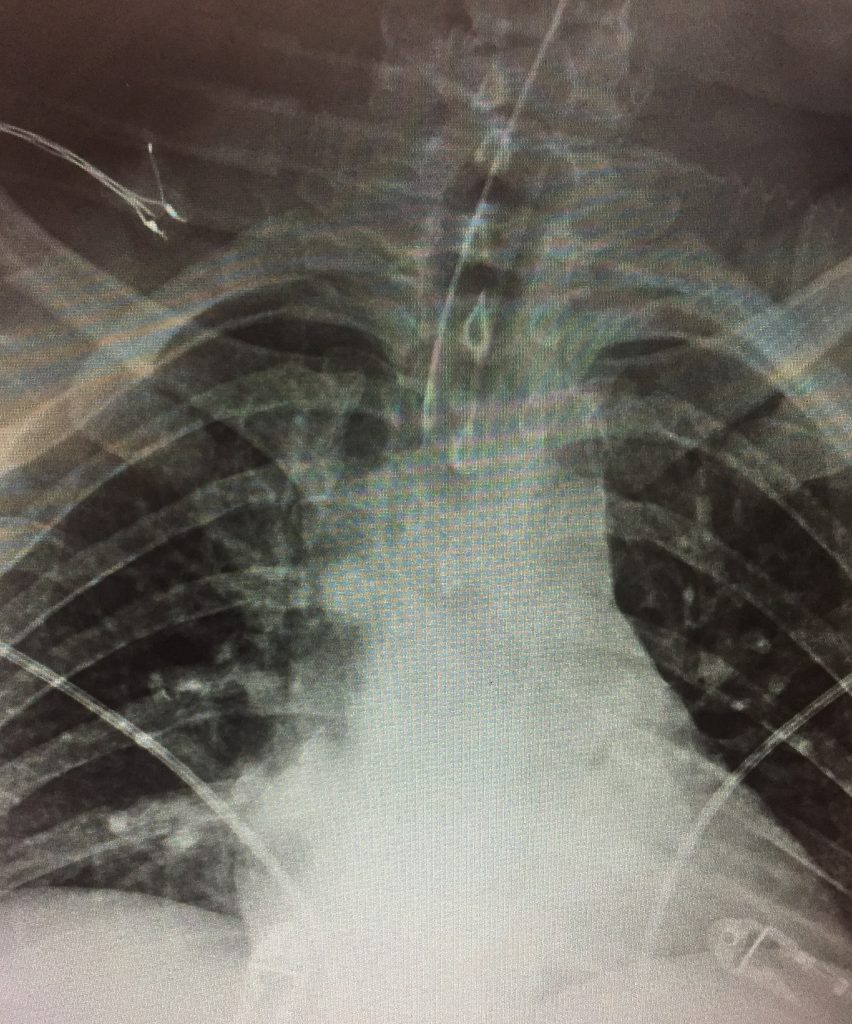
I asked the x-ray tech to shoot a plain film of the neck and here’s what I saw:

It was laying about 7cm above the carina. The tube was advanced and repeat x-ray is shown below:
Learning points:
- Teaching is great, but it requires one to be extra-vigilant
- Always always always remember to check your post-intubation films in a timely manner. Can you imagine if this patient had gone upstairs with the tube 7cm above the carina?



{kind=link}