
A young healthy person was involved in a high-speed MVA. She arrived with positive ‘seat-belt’ signs and complaining of pain in the chest and abdomen. On exam, her trachea was mid-line, breath sounds clear bilaterally, and vital signs normal. Given the high concern for potential injury, a very quick bedside FAST failed to show any obvious intra-peritoneal free fluid.
Chest and pelvis x-rays, CT chest, and CT abd/pelvis are ordered. Somehow (!) the patient was whisked away to CT so those scans were done before the x-rays; the following scout image is obtained:


Here’s a short video scrolling through the CT scan:
If the video won’t work, here’s a still image from the scan:
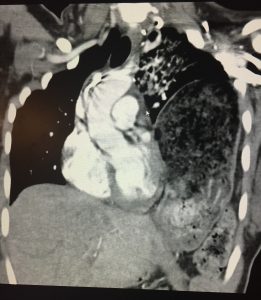
Final diagnosis: “Large traumatic left diaphragmatic rupture with herniation. Dilated stomach, pancreas, spleen, and splenic flexure all within the thoracic cavity. Perisplenic hematoma. Small left-sided pneumothorax.”
With regard to diaphragmatic ruptures, the postero-lateral left side is more commonly involved in blunt trauma since the liver provides some degree of protection to the right side. Mortality rates in isolated diaphragmatic ruptures are reported as 15-20%.
In penetrating trauma (most often GSWs and stab wounds), smaller defects are created with high probability for later obstruction/strangulation.
Management involves placing an NG tube to decompress the stomach – this can potentially improve respiratory status. Ultimately, patients will need a laparotomy for repair. Of course, associated injuries should be managed and ATLS protocols followed.



{kind=link}